The final day of the BRCA Symposium held three unique sessions, covering the search for new breast cancer genes, risk assessment, and a closing session in memory and honor of Marla Miller. In 2003, Marla Miller passed away from metastatic breast cancer after testing positive for a BRCA1 mutation. Marla's sister, Joanne Miller-Eisman, founded the
Hereditary Breast and Ovarian Cancer Foundation with the aim of spreading awareness of HBOC, raising funds for HBOC research, and ultimately, providing BRCA1/2 carriers with better options and outcomes. They have done and continue to do incredible work, and are instrumental to the organisation of the BRCA Symposium. Joanne Miller-Eisman gave a moving message to end the conference, where her passion for helping those with HBOC shined brightly.
 |
Dr. Ian Campbell from Australia gave an excellent presentation on gene candidates of breast cancer susceptibility. In their study, Dr. Campbell and his colleagues found clear evidence of variants in the gene PALB2 conferring increased risk for breast cancer. Pathogenic variants in a gene called RAD51C were found to predispose to triple negative breast cancer, while there was evidence for homozygous (two copies of) NTHL1 variants leading to increased breast and colon cancer risks. Dr. Campbell strongly emphasized that not only are individual genes important in assessing cancer risk, but we must also look at the genomic context.
Another engaging talk in the day's first session was by Dr. Laura Ottini from Italy, who focused her presentation on male breast cancer patients. Many people are surprised to find out that men can get breast cancer too. In fact, according to Dr. Ottini, 1% of breast cancer cases occur in males. Dr. Ottini and her colleagues analysed 503 male breast cancer cases in Italy where the man had tested negative for a BRCA1/2 mutation. They wanted to identify variants in other genes that may have caused this increased breast cancer risk. The researchers found pathogenic variants in 14 genes other than BRCA1/2, suggesting that hereditary breast cancer is much wider than BRCA1/2 alone. |
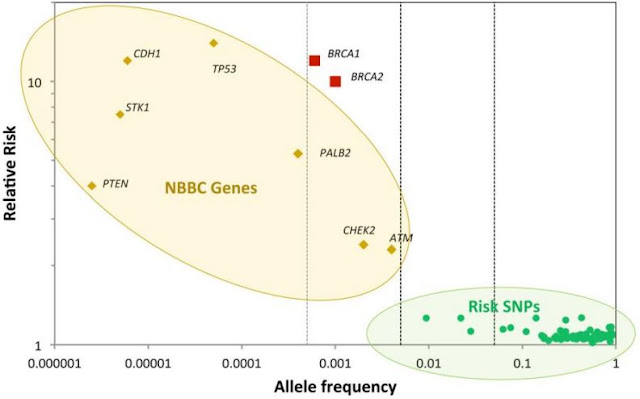 |
| The image above came up in a few presentations, and was originally published in the New England Journal of Medicine in 2015 by Easton and colleagues. NBBC in the left oval stands for non-BRCA1/2 breast cancer risk genes. As you can see in the graph, BRCA1 and BRCA2 are outliers, as they confer high relative breast cancer risk and variants occur more frequently than in other genes represented. What is also interesting is the group in the lower right-hand corner. This group consists of single nucleotide polymorphisms (SNPs), referring to a single base change in the DNA. Although these SNPs confer a low relative risk for breast cancer, they occur quite frequently in the population. Additionally, they may interact with other SNPs, resulting in a greater breast cancer risk. This knowledge has led to many researchers seeking to incorporate a "polygenic risk score" into risk assessment for breast and ovarian cancer. In the day's second session, Dr. Antonis Antoniou from Cambridge gave an exciting talk on incorporating a polygenic risk score into risk assessment. For example, Dr. Antoniu explained how a man with a BRCA1 mutation has around a 30% risk of developing prostate cancer. However, the risk also depends on SNPs (and therefore a polygenic risk score), and because of this, incorporating this score into risk assessment would assist in more accurate risk prediction. |
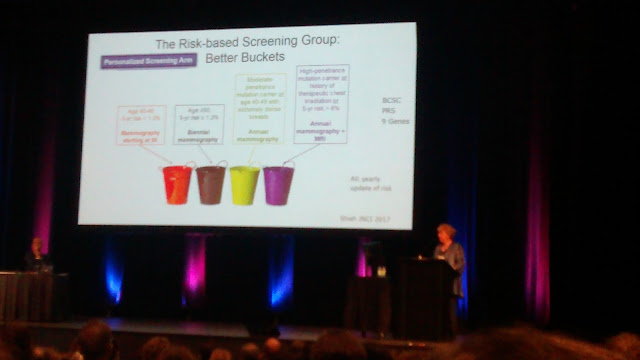 |
The above image is of Laura van't Veer from California giving an intriguing talk on WISDOM (women informed to screen depending on measures of risk). The basis of "personalized screening" is that women would receive screening based on their personal level of risk, where women in the lowest risk category may receive mammography every two years (or less!) There is certainly some interesting discussion around this approach, and I'm intrigued to look further into Dr. van't Veer's work.
Dr. Mary-Claire King gave the final talk of the conference in honor of Marla Miller. In 1990, Dr. King's lab was the first to link a gene (BRCA1) to breast cancer susceptibility. There were many things I could point to about Dr. King's talk, but the component that stood out to me the most was her commitment and genuine passion for helping people through science. She was kind and honest, yet radiated immense knowledge collected from decades of research. Dr. King has been working with a family since the 1970s where there had been five (yes, 5!) cases of male breast cancer.
|
 |
| To paraphrase the words of Mary-Claire King: the race is not over until no one has to die of breast or ovarian cancer. There is much work to be done, but I'm thankful to have seen the incredible work being done internationally to conquer HBOC. Much progress has been accomplished and much progress still lies ahead. This conference has inspired and challenged me. I was inspired by the immense amount of work that has been done to better patients' lives, yet challenged by the fact that so much is still unknown. We need to keep asking questions and never be afraid to look at things with a fresh perspective. |
I hope you have enjoyed these posts on my experience in Montreal at the BRCA Symposium 2018. It was an amazing conference that I will look back on with great joy. Thank you to UFV for providing me with generous funding to make this trip possible, and to my amazing supervisors Angela Bedard, James Bedard, and Intan Schrader for encouraging me to submit an abstract and attend this fantastic meeting!
When opportunities of a lifetime come your way, look them in the eye, hold on tight, and go for it!
~ Vivienne






Comments
Post a Comment